
Table 1: A summary of the strength of evidence
Tibial Diaphyseal Fracture Rates Following Tibial Tuberosity Advancement Rapid (TTAR) and Traditional Tibial Tuberosity Advancement (tTTA)
a Knowledge Summary by
Wye Li Chong BVSc, MANZCVS 1*
1Canberra Veterinary Emergency Service, 21 Crinigan Cir, Gungahlin, ACT, 2912, Australia
*Corresponding Author (wyechong@gmail.com)
Vol 4, Issue 1 (2019)
Published: 05 Mar 2019
Reviewed by: Geoff Robins (BVetMed, FACVSc) and Yves Samoy (DVM, PhD, DipECVSMR)
Next review date: 05 Mar 2021
DOI: 10.18849/VE.V4I1.179
In dogs with cruciate disease, is the use of TTA Rapid (TTAR) compared to traditional TTA (tTTA) associated with a higher risk of tibial diaphyseal fractures?
Clinical bottom lineBased on studies published between January 2013 and January 2018, the rate of tibial diaphyseal fractures as a complication of Tibial Tuberosity Advancement Rapid (TTAR) surgery is within the published limits of traditional Tibial Tuberosity Advancement (tTTA). In this period, seven studies were related to tTTA, comprising of four; one case series, two retrospective case-control studies, and one retrospective cohort study. Five case series were related to TTAR. All evidence within this period has been observational (Level 3 and 4 evidence). No direct head-to-head comparison between the techniques has been studied.
The evidence
Based on a literature search of the last 5 years (prior to 23 January 2018), there were seven PICO related studies for tTTA and five for TTAR. Of the articles for tTTA, 3/7 were retrospective case series, 1/7 prospective case series, 2/7 retrospective case-controls and 1/7 retrospective cohort study. All TTAR studies were case series.
Summary of the evidence
| Population: | Dogs |
| Sample size: | 1613 |
| Intervention details: |
|
| Study design: | Retrospective case-control study |
| Outcome Studied: | Major complication rates in dogs receiving tibial tuberosity advancement surgery and the effects of medial meniscal release on postoperative meniscal tear. |
| Main Findings (relevant to PICO question): |
Major complication rate – 13.4%
Minor complications – not included Medial meniscal tear 40.5% had medial meniscal injury and were treated with partial meniscectomy 59.4% had normal meniscus. 72.4% of these dogs had meniscal release. 0.5% of these dogs developed postliminary meniscal injury. 27.6% of dogs with normal meniscus did not receive meniscal release. 10.2% developed postliminary meniscal injury. Postoperative patellar luxation 1.2% developed patellar luxation postoperatively. Surgical site infection 6.9% of dogs developed superficial surgical site infection All were managed successfully with conservative treatment. 1.1% developed deep SSI necessitating surgical intervention. Implant failure and fractures 1% of dogs had implant failure requiring revision surgery. 0.7% (11 dogs) developed fracture; 3/11 tibial diaphyseal fractures and 8/11 tibial tuberosity fracture. PICO – three (0.18%) tibial diaphyseal fractures were reported. |
| Limitations: |
|
| Population: | Dogs receiving single-session bilateral plated tibial tuberosity advancement. |
| Sample size: | 148 stifle joints |
| Intervention details: | Single stage bilateral traditional TTA.
68 tTTAs were performed with forked plates. 75 tTTAs were performed with screw plates. |
| Study design: | Retrospective case series |
| Outcome Studied: | Short-term radiographic complication rates and healing scores in bilateral single-session TTAs. |
| Main Findings (relevant to PICO question): |
Overall radiographic complication rates of 17.6% (13/72 dogs), of which only one dog was considered to have major complications.
Minor complications in 12 dogs include forked plate displacement (6), tibial tuberosity fracture (4), screw failure (2) and cage displacement (1). Forked plates had greater complications compared to screw plates. Four stifle joints had tibial tuberosity fractures. PICO – One stifle joint had tibial diaphyseal fractures (0.007%). |
| Limitations: |
|
| Population: | 122 dogs |
| Sample size: | 167 stifle joints |
| Intervention details: |
|
| Study design: | Retrospective case series |
| Outcome Studied: |
|
| Main Findings (relevant to PICO question): |
Minor complications in 14/167 (8%)
Major complications in 15/167 (9%)
Overall success rate is 91% over 167 procedures. 22 procedures were required before the published veterinary surgeon became acceptably competent to perform tTTA and have complications within published ranges. PICO – 0 dogs had tibial diaphyseal fractures. |
| Limitations: |
|
| Population: | Boxer vs. non-Boxer dogs with cruciate disease |
| Sample size: | 36 Boxer stifle joints and 271 non-Boxer stifle joints |
| Intervention details: | All dogs received forked plate TTA Meniscus:
Antibiotics:
|
| Study design: | Retrospective cohort study |
| Outcome Studied: | Incidence of major and minor complication rates associated with tTTA in Boxers vs. non-Boxers. |
| Main Findings (relevant to PICO question): |
|
| Limitations: |
|
| Population: | Dogs that underwent single-stage bilateral plated TTA vs. unilateral plated TTA |
| Sample size: | 44 (88) bilateral TTA (bTTA) vs. 86 unilateral TTA (uTTA) |
| Intervention details: | All dogs received plated TTA system – manufacturer undefined. All dogs received commercial synthetic or cancellous bone graft on osteotomy site. Some dogs received external coaptation (number undefined). All dogs were re-evaluated at:
|
| Study design: | Retrospective case-control |
| Outcome Studied: | Major and minor complication rates of bTTA compared to uTTA at 4 and 8 weeks postoperatively. Major complications defined as complications requiring further surgery. Minor complications defined as any other complications. |
| Main Findings (relevant to PICO question): |
Major complication rates (no significant difference)
bTTA 11/88 (12.5%) vs. uTTA 2/86 (2.3%) Minor complication rates (significantly different) bTTA 23/88 (26.1%) vs. uTTA 21/86 (24.4%) Overall complication rate (no significant difference) bTTA 31/88(35.2%) vs. uTTA 21/86 (24.4%) Fracture bTTA – 2/88 tibial diaphyseal fracture and 9/99 tibial tuberosity fracture uTTA – 1/88 tibial tuberosity fracture
PICO – 2/88 (2.3%) tibial diaphyseal fracture in bTTA and 0/88 in uTTA |
| Limitations: |
|
| Population: | Skeletally mature dogs > 17 kg |
| Sample size: | 24 dogs |
| Intervention details: |
|
| Study design: | Prospective case series |
| Outcome Studied: | Complications, lameness, thigh circumference, range of motion, radiographic osteoarthritis at 6 weeks, 6 months, and 1 year. |
| Main Findings (relevant to PICO question): |
Postoperative complications 8/24 (33.3%)
PICO – 0 dogs had tibial diaphyseal fracture. |
| Limitations: |
|
| Population: | Large breed dog > 50kg |
| Sample size: | 145 stifle joints |
| Intervention details: | 91 stifle joints received Securos Surgical TTA XGEN plated system
54 stifle joints received Tibial Plateau Leveling Osteotomy (TPLO) |
| Study design: | Retrospective case-control |
| Outcome Studied: | Major and minor complication rates of TTA compared to TPLO in large breed dogs. The null hypothesis is that there is a difference in major complications between the two techniques, based on medical records. |
| Main Findings (relevant to PICO question): |
TTA group Overall complication – 33% Major complication rate 18/91 (19.8%)
Minor complication rate – 13/91 (13.2%)
PICO – 1/91 (1.1%) cases had tibial diaphyseal fracture
TPLO group Major complications – 15/54 (27.8%)
Minor complication – 12/54 (22.2%)
|
| Limitations: |
|
| Population: | Dogs with cruciate disease |
| Sample size: | 141 clinically lame dogs, 152 stifle joints |
| Intervention details: |
|
| Study design: | Case series |
| Outcome Studied: | Subjective evidence of lameness and complications by clinical assessment at 3 months, and validated questionnaire at >6 months postoperatively. |
| Main Findings (relevant to PICO question): |
PICO – 1/152 (0.66%) developed tibial diaphyseal fracture treated by internal fixation. |
| Limitations: |
|
| Population: | Dogs with unilateral cruciate disease |
| Sample size: | 50 dogs |
| Intervention details: |
|
| Study design: | Prospective case series |
| Outcome Studied: | Outcomes, minor and major complication rates. |
| Main Findings (relevant to PICO question): |
PICO – 0% of dogs developed tibial diaphyseal fracture |
| Limitations: |
|
| Population: | Small breed dog – mean weight 9 kg (4.8–15 kg) |
| Sample size: | 48 stifle joints |
| Intervention details: |
|
| Study design: | Retrospective case series |
| Outcome Studied: | Lameness and postoperative complications at 6 weeks were measured by clinical examination and owner questionnaire assessment at mid- to long-term follow up (median 72 weeks). |
| Main Findings (relevant to PICO question): |
PICO – 2/48 (4.17%) developed tibial diaphyseal fracture |
| Limitations: |
|
| Population: | Dogs receiving TTAR |
| Sample size: | 17 |
| Intervention details: |
|
| Study design: | Case series |
| Outcome Studied: | Minor complications and major complications. Lameness and pain assessment 1, 2 and 3 months postoperatively. |
| Main Findings (relevant to PICO question): |
PICO – 0/17 stifle joints receiving TTAR resulted in tibial diaphyseal fracture. |
| Limitations: |
|
| Population: | Dogs that received plateless TTA with complications of tibial diaphyseal fracture |
| Sample size: | 17 dogs; 11/17 received Orthofoam–MMP procedure, 6/17 received TTAR procedure |
| Intervention details: | All 17 dogs received revision surgery to correct tibial tuberosity fracture by various forms of internal fixation. |
| Study design: | Case series |
| Outcome Studied: | Outcome, major and minor complication following repair of tibial diaphyseal fracture secondary to complication of plateless TTA techniques. |
| Main Findings (relevant to PICO question): |
PICO
|
| Limitations: |
|
Appraisal, application and reflection
Since the advent of tTTA in 2002 (Montavon et al., 2002), various second generation TTA procedures have been invented. These techniques (TTAR, Orthofoam-MMP, MMT, TTA–2) utilise custom saw guides to aid the surgeon in producing an incomplete osteotomy of the tibial tuberosity. They have different implant designs, and they eliminate the use of a supporting plate (Ness 2016 Samoy et al., 2015, Bleakley 2015, Brunel et al., 2013). These techniques are generally aimed at the non-specialist surgeon and are marketed to be simpler than tTTA while offering comparable results. A recent case series of 17 dogs (de Sousa et al, 2017) suggests that tibial diaphyseal fractures may be a well-recognised catastrophic complication of second generation TTA techniques. However, the study design could not evaluate the actual incidence or prevalence of this complication.
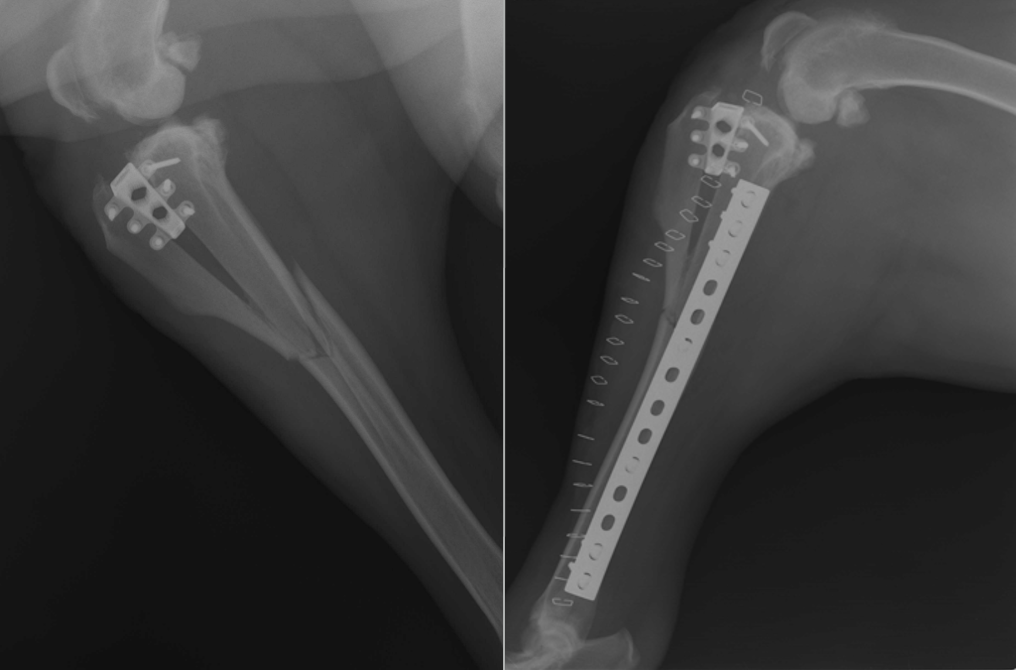
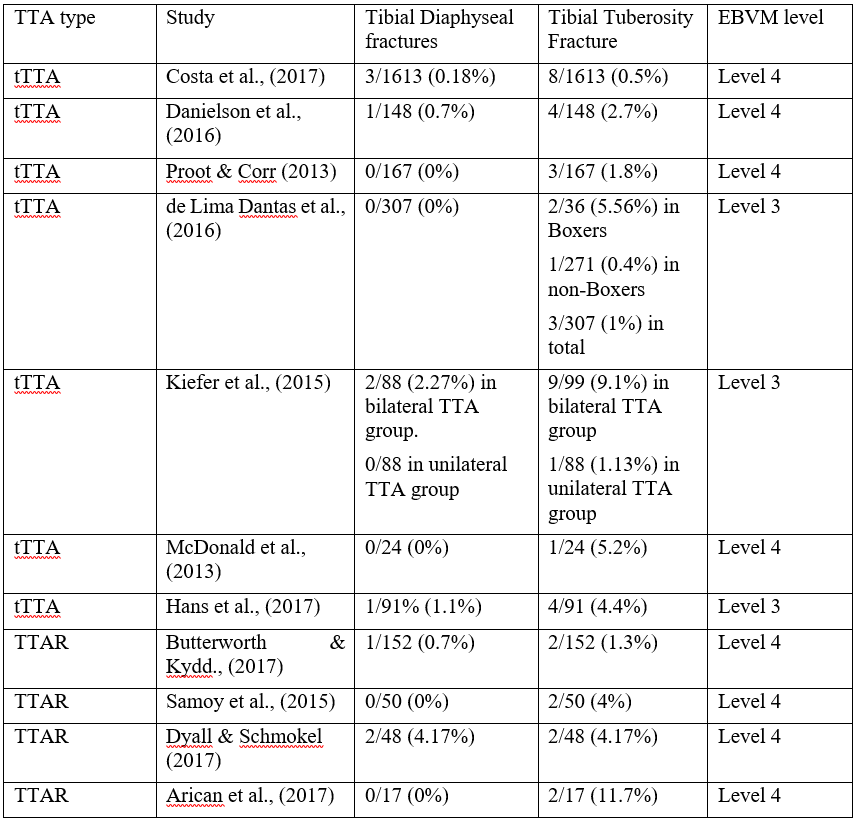
From this table, the rate of tibial diaphyseal fractures from tTTA (0–2.3%) compared to TTAR (0–4.17%) are roughly comparable. In the TTAR group, Dyall & Schmokel’s (2017) report of 4.17% tibial diaphyseal fractures using TTAR on small breed dogs (< 15 kg) was notably higher than the other three studies. The higher fracture rate was attributed to the relatively large cage size, which may have overwhelmed the elasticity of the cranial tibial cortex, predisposing to fracture. If small breed dogs were excluded from the comparison then the rate of tibial diaphyseal fractures for TTAR would be 0–0.7%, which is within the published limits for tTTA (0–2.3%). A two-tailed T test (https://www.socscistatistics.com/tests/studentttest/Default2.aspx) comparing TTAR (0, 0, 0.7, 4.17) vs tTTA (0.18, 0.7, 0, 0, 2.27, 0, 1.1) reveals t-value of 0.7246 and p-value of 0.487105, showing a lack of significance at p < 0.05, although the sample size is very small.
Interestingly, tibial tuberosity fractures, while not directly related to the PICO, occur more commonly across studies. In tTTA, a complete osteotomy of the tuberosity is held in place by a forked or screw plate. Fractures are generally attributed to poor plate and cage positioning, as well as narrow tuberosity width postosteotomy (Costa et al., 2017). In TTAR, the osteotomy is incomplete leaving the distal hinge intact. Fractures through the distal hinge were considered as tibial tuberosity fractures across the TTAR studies (Butterworth & Kydd (2017), Samoy et al., (2015), Dyall & Schmokel (2017), Arican et al., (2017)). Despite the added risk of the distal hinge fracture for TTAR, the tibial tuberosity fracture rate of 0.5–9.1% for tTTA and 1.3–11.7% for TTAR does not differ significantly at p < 0.05, with two-tailed T test showing t-value of -0.91676 and p-value 0.378929. In addition, the 2/50 tibial tuberosity fractures in Samoy et al. (2015) happened before the development of a dedicated saw guide. The TTAR has since been modified to exclude the use of the Maquet hole at the distal end of the incomplete osteotomy while utilising a longer osteotomy. This is facilitated by a dedicated saw guide, allowing an accurate cut. It is yet unknown if this will lead to reduced tuberosity and diaphyseal fractures.
Proot & Corr’s (2013) clinical audit suggests that it takes 22 tTTA procedures to gain acceptable competence. To date, a similar clinical audit has not been published for TTAR and it is unknown if major complications such as tibial fractures are more common in the hands of inexperienced veterinary surgeons. It is also unclear from the data how often tibial fractures are due to faults in the technique or faults in the postoperative care.
It should be noted that all evidence that met the inclusion criteria for this PICO is of low grade evidence and to date no head-to-head control trials have been done comparing tTTA to TTAR or other second-generation plateless techniques. Future studies could focus on which perioperative factors might have an impact on fracture complications. For example, the experience of the veterinary surgeon, the use of bone grafting, which may accelerate healing, the size and age of the patient, which may influence bone elasticity, as well as owner compliance and protective effect of external coaptation in the early postoperative period. Based on current evidence however, the rate of tibial fractures does not differ between tTTA and TTAR. Until data to the contrary becomes available, veterinary surgeons performing either technique should be cognizant of their ability to perform complex osteotomy, as well as audit their complications and compare them against published limits.
Methodology Section
| Search Strategy | |
| Databases searched and dates covered: | CAB Abstracts on OVID Platform 1973–Week 4 2019
Pubmed |
| Search terms: | (canin* or dog*) and (cruciate) and (tibial tuberosity advancement or TTA) or (TTA Rapid) and (fracture* or complication*) |
| Dates searches performed: | 22/01/2018 |
| Exclusion / Inclusion Criteria | |
| Exclusion: | CAB Abstracts via the Ovid platform covering from 1973 to 2013 weeks 1.
Pubmed with publication dates > 5 years Non-english articles Articles with contents irrelevant to PICO. |
| Inclusion: | All TTAR papers and tTTA related papers with data pertaining to tibial fractures and complications. |
| Search Outcome | |||||
|
Database |
Number of results |
Excluded – non English |
Excluded – publications > 5 years old |
Excluded – irrelevant to PICO |
Total relevant papers |
|
CAB Abstracts |
48 | 11 | 15 | 10 | 12 |
|
Pubmed |
37 | 0 | 17 | 11 | 9 |
|
Total relevant papers when duplicates removed |
12 | ||||
The author declares no conflicts of interest.
Intellectual Property Rights
Authors of Knowledge Summaries submitted to RCVS Knowledge for publication will retain copyright in their work, and will be required to grant to RCVS Knowledge a non-exclusive licence of the rights of copyright in the materials including but not limited to the right to publish, re-publish, transmit, sell, distribute and otherwise use the materials in all languages and all media throughout the world, and to licence or permit others to do so.
Disclaimer
Knowledge Summaries are a peer-reviewed article type which aims to answer a clinical question based on the best available current evidence. It does not override the responsibility of the practitioner. Informed decisions should be made by considering such factors as individual clinical expertise and judgement along with patient’s circumstances and owners’ values. Knowledge Summaries are a resource to help inform and any opinions expressed within the Knowledge Summaries are the author's own and do not necessarily reflect the view of the RCVS Knowledge. Authors are responsible for the accuracy of the content. While the Editor and Publisher believe that all content herein are in accord with current recommendations and practice at the time of publication, they accept no legal responsibility for any errors or omissions, and make no warranty, express or implied, with respect to material contained within. For further information please refer to our Terms of Use.