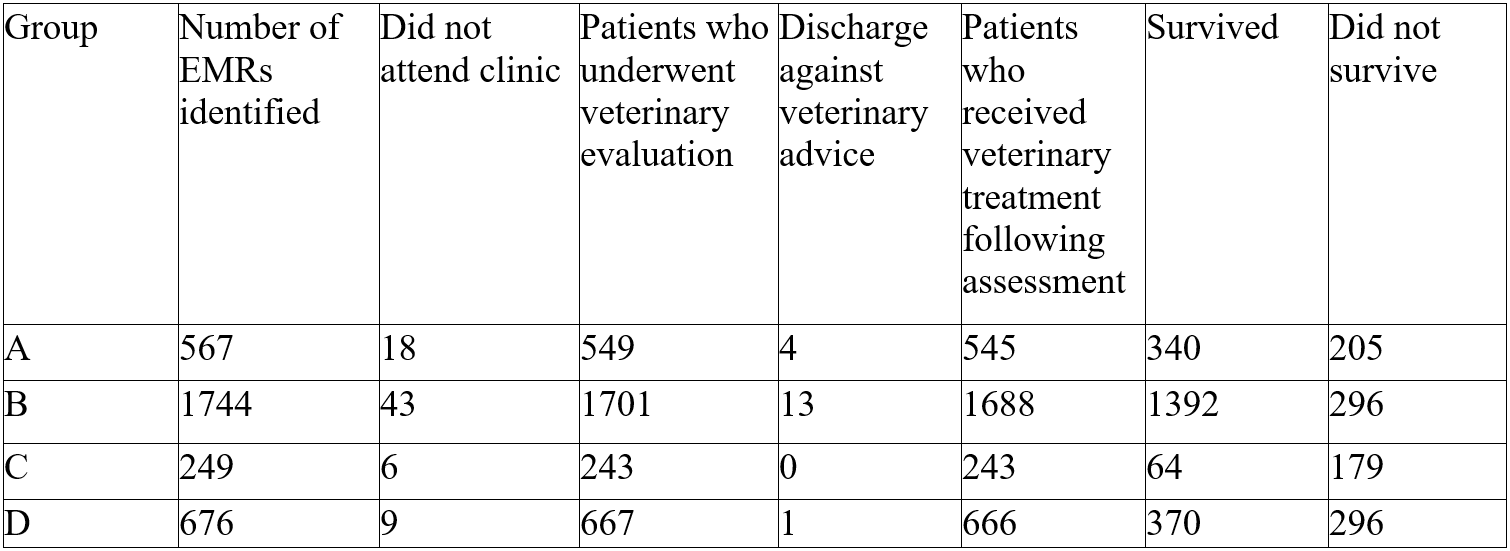
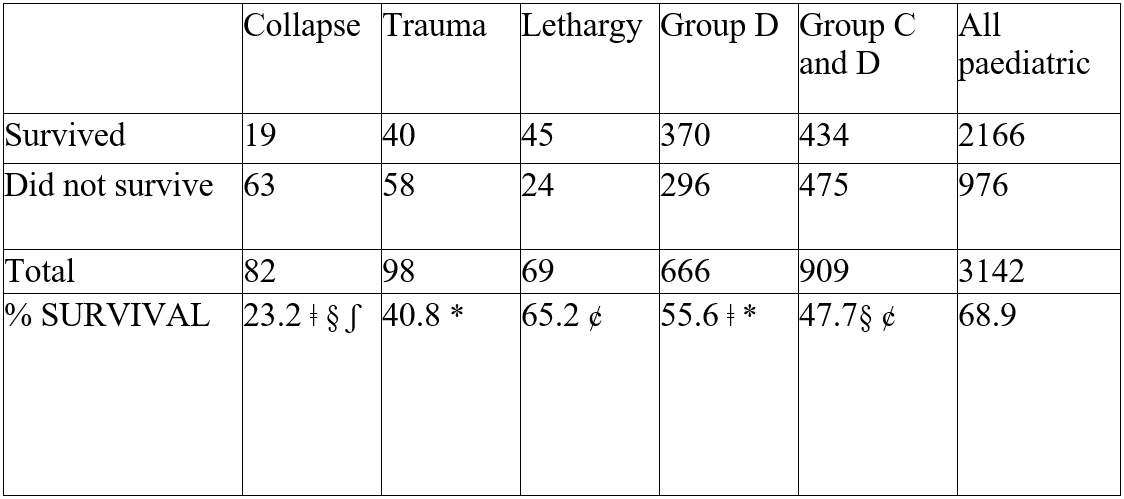
Table 1: Outcome recorded for all canine/feline patients whose owners contacted the out-of-hours clinics for advice
Survival and Presenting Complaint of Canine and Feline Paediatric Emergencies Presenting to UK Emergency Clinics
Emma Donnelly BSc. (Hons), BVMS, MRCVS1*
1Vets Now, 123 North Street, Glasgow, G3 7DA
2University of Melbourne Veterinary Hospital, 250 Princes Highway Werribee, Victoria 3030, Australia
*Corresponding Author (Emma.Donnelly@vets-now.com)
Vol 3, Issue 3 (2018)
Published: 04 Jul 2018
Reviewed by: Bruce Smith (BVSc MS FANZCVS DACVS) and Shailen Jasani (MA VETMB MRCVS DACVECC)
DOI: 10.18849/VE.V3I3.174
Objective: To describe the presenting problems for paediatric dogs and cats presented to emergency clinics, and to determine what factors influence mortality.
Background: There is a lack of published literature available on canine and feline paediatric emergencies, their survival rates and factors that contribute to mortality. Experience and opinion largely replace evidence-based medicine when treating this subset of the emergency population.
Evidentiary value: Evidentiary value for primary and emergency care practitioners is strong as the data is based on a large primary emergency care database. The paediatric population analysed consisted of 3142 paediatric canine and feline patients.
Methods: A retrospective review of canine and feline emergency admissions to emergency out-of-hours clinics (May 2012-January 2014) was conducted. Data recorded included age, nature of complaint, euthanasia/death during treatment, and survival to discharge. Survival to discharge included all patients who presented to the clinic for examination, received treatment and were subsequently discharged; this includes those patients who were discharged home or to their primary vets care. Patients were divided into four groups: canine patients ≤ 3 months of age and 3-6 months and feline patients ≤ 3 months of age and 3-6 months.
Results: Paediatric patients represented around 3% of the emergency cases identified in the database. Survival to discharge in patients ≤3 months of age was significantly reduced in comparison to patients between 3-6 months of age, in both species. Feline paediatric patients had reduced survival to discharge compared to their canine counterparts.
Conclusion: Paediatric patients have a low survival rate, indiscriminate of species and reason for presentation, with lower survival in younger animals; with a significant difference in survival between canine and feline patients.
Application: The results of this study are important to small animal veterinarians in both emergency and non-emergency practice.
Paediatric and neonatal patients are intrinsically less able to adapt and respond to changes and insults. In the author’s opinion, this group frequently presents to out-of-hours clinics as emergency patients. However, there is no epidemiological data available to confirm this. Although there is no universally agreed nomenclature, generally speaking, patients between two and six weeks are referred to as infants, between six and 12 weeks as weanlings and those between 12 weeks of age and six months are referred to as juvenile patients (Mathews 2005). In more general nomenclature, the term ‘neonate’ describes those from birth to two weeks of age while ‘paediatric’ describes those from two weeks to six months (McMichael 2015). Given this lack of consensus in the nomenclature, but the commonly accepted observation that dogs and cats <6 months of age represent an easily identified, immature population, for the purposes of this article we will describe all dogs and cats <6 months of age as ‘paediatric’.
Paediatric and neonatal canine and feline patients have low body energy reserves, an immature physiology, an altricial (or highly dam-dependent) nature and a high metabolic rate, which can lead to rapid changes in their clinical status and subsequent presentation in a critical condition (Gunn-Moore 2006; Centre et al. 1995). They also have a developing immune system and so are inherently more susceptible to infectious disease (Munnich et al. 2014). In comparison to adult canine and feline patients, their altered physiology and the differing underlying aetiologies of conditions can also complicate clinical examination and treatment decisions (McMichael 2015).
Feline and canine neonatal and paediatric patients are tachycardic in comparison to their adult counterparts, with a normal paediatric heart rate being around 200 bpm for puppies and 250 bpm for kittens. They also have lower blood pressure than adult patients (Magrini 1978); however, their blood pressure increases as their sympathetic nervous system matures over the first few months of life. In the canine patient, mean arterial blood pressure does not reach a ‘normal’ adult value until around nine months of age. At one month of age, a systolic pressure of 48mmHg is thought to be normal (Magrini 1978); this is not only lower than that of adults but below even the mean arterial pressure at which impaired tissue perfusion is often considered to be occurring in most adult patients (Cooper 2015). Auscultation of the lungs of paediatric patients can be complicated by their increased respiratory rate and inherently higher interstitial fluid content (Tonneson et al. 2012), leading to normal breath sounds being interpreted as adventitious. Such differences in the respiratory and cardiovascular systems can complicate assessment of perfusion in these patients. A prospective study in 68 puppies and 30 adult dogs revealed that lactate has the potential to be a suitable marker of hypoperfusion (McMichael 2005). However, as with other haematological and biochemical values, adult reference ranges cannot be applied to neonatal dogs and cats. A definitive reference range for lactate has not yet been established.
Physiological and behavioural responses to critical illness differ from adult patients, sometimes masking the severity of the situation; this disparity is described well in human paediatric medicine (Woollard et al. 2004), although it is often under-emphasised in the veterinary literature. A thorough understanding of small animal paediatric patients’ clinical, haematological, biochemical and pharmacological differences from their adult counterparts is vital in triaging, stabilising and treating such patients. In human medicine there is recognition of the limitations of treating paediatric patients in an adult-focused environment and as such paediatric emergency and critical care has become a separate sub-speciality (RCPH, 2008).
There is little published literature available for paediatric and neonatal veterinary patients, particularly dogs and cats. In canine neonatal patients, infectious diseases are the second leading cause of mortality (Nielen 1988). A limited number of case reports for small animal neonatal patients can be found in the literature, however, to the authors’ knowledge, there are no large-scale epidemiological studies available (Chellani et al. 1985; Gupta, et al. 1996). A greater body of literature exists for neonatal disease in other species, such as horses, perhaps due to their perceived greater individual value. The mortality rate of adult canine and feline patients presenting to out-of-hours emergency practice has been reported as 11.9% and 20.2% respectively (Firth et al. 2014), however no such data has as yet been explored for paediatric patients.
Given these differences between paediatric and adult patients and due to the lack of literature available, this study aimed to identify the most common causes for presentation of canine and feline paediatric patients to a group of emergency out-of-hour clinics, to ascertain the survival to discharge for such patients and to determine whether factors such as the presenting complaint or age influence survival.
Data collection:
The electronic medical record (EMR) database of 50 dedicated emergency clinics between May 2012 and January 2014 was used as the data source. All emergency clinics use the same centralised clinical records system1 on which the data of all patients who contact the clinics is recorded; first contact with the clinic is primarily by telephone . All canine and feline paediatric patients (defined as less than six months of age at the time of presentation) were identified and the following information was recorded for the patients who contacted the clinics: species, age, presenting complaint and outcome. Presenting complaint was coded using standardised nomenclature (VeNOM) accessed via a drop-down menu in the electronic medical record. The responsible clinician for each patient selected the most appropriate presenting complaint; the computer software allows one complaint to be recorded for each patient. The paediatric patients who did not present to a clinic following initial contact and those who presented but were subsequently discharged against veterinary advice with no further treatment were excluded from the study.
Outcome was recorded as survival to discharge or non-survival (including death during hospitalisation, dead-on-arrival and euthanasia). For analysis, the patients were further subdivided into species and then into age groups: those ≤3 months of age at presentation (canine - Group A, feline - Group C) and those between three and six months of age at presentation (canine - Group B, feline - Group D).
Statistical analysis:
Descriptive statistics and chi-square analysis was performed using a standard software package2 to compare survival to discharge versus non-survival between canine (Groups A and B) and feline patients (Groups C and D), between inter-species cohorts (Groups A and B vs Groups C and D) and the presenting complaint of all patients (Group A, B, C and D).
A total of 119261 emergency canine and feline cases contacted the clinics during the studied period; of these, 81241 patients were canine, and 38020 were feline. A total of 3236 of these patients were paediatric as previously defined: 2311 were puppies, and 925 were kittens. Ninety-seven percent of canine paediatric patients (2250/2311) and 98% of feline patients (910/925) presented for examination. Patients who did not present to the clinic or presented to the clinic but were discharged against veterinary advice were excluded from further study (Table 1).
Patients that underwent further veterinary evaluation were grouped according to species and their age at presentation. Group A (dogs ≤ 3months of age at presentation) and Group B (dogs 3-6 months) consisted of 545 and 1688 puppies respectively. Group C (cats ≤ 3months) and Group D (cats 3-6 months of age) contained a total of 243 and 666 kittens. There was no statistically significant difference between contact and subsequent presentation to the clinic between species (p=0.8).
Group A
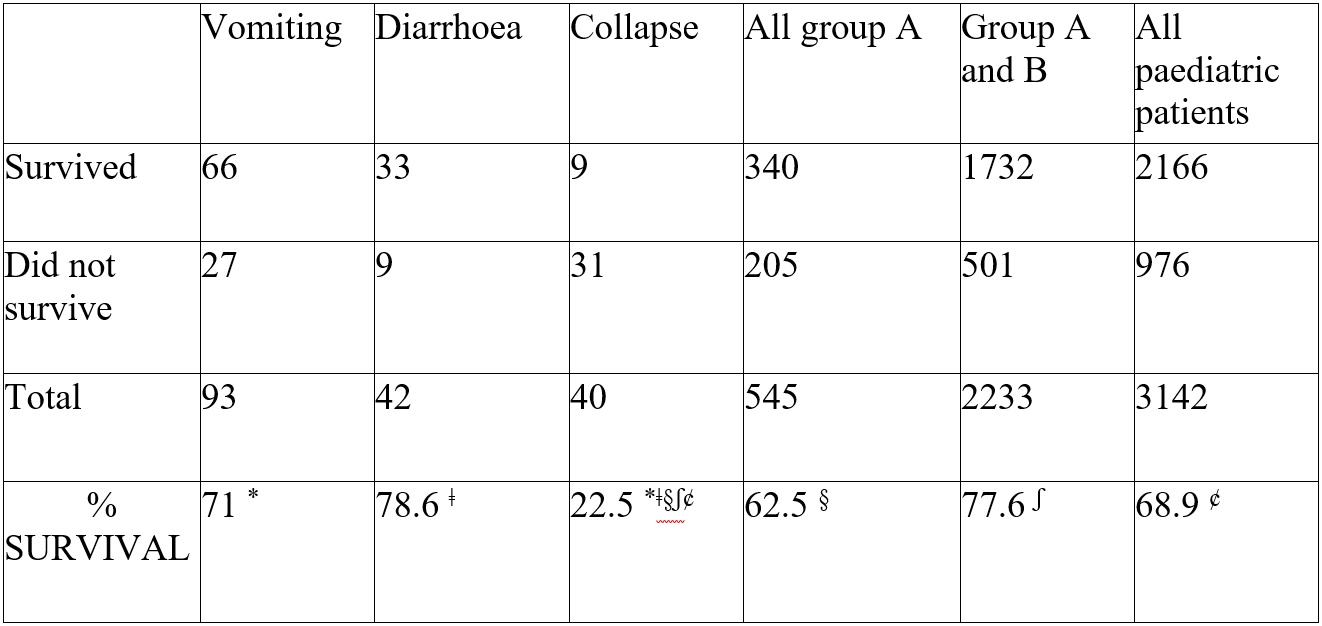
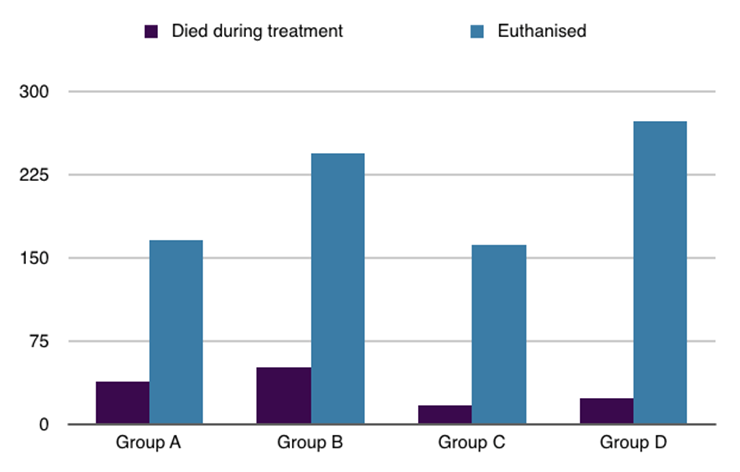
Group A’s overall survival was 62.5% (Table 1). The three most common presenting complaints were vomiting (17%), diarrhoea (8%) and collapse (7%). Patients who presented for vomiting had a survival rate of 71% while those presenting for diarrhoea had a survival rate of 78.6%. Group A patients presenting with vomiting and diarrhoea were not significantly less likely to survive than the other paediatric patients However, those who presented collapsed had a significantly lower survival rate (22.5%) than other paediatric patients irrespective of age, species or presenting complaint (Table 2) (p<0.001). Of the patients who did not survive to discharge in Group A, 81% were euthanised (Figure 2).
Group B
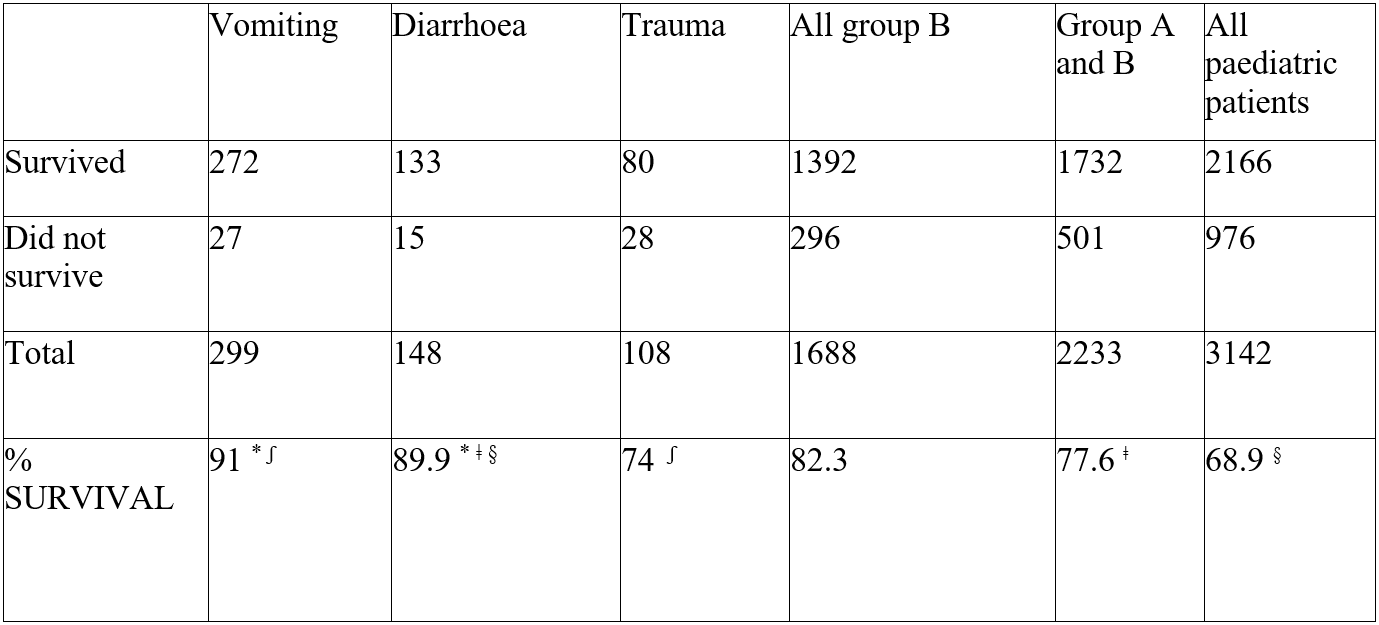
Group B’s overall survival was 82.3%. The three most common presenting complaints were vomiting (18%), diarrhoea (9%) and trauma (7%). Patients who presented for vomiting had a survival rate of 91%; this was significantly higher than puppies within the same age category presenting with other complaints (p <.001). Patients in Group B presenting for diarrhoea had a survival rate of 89.9%; this was significantly higher than paediatric patients in Groups A, C and D (p <.001). However, these patients (Group B patients presenting for diarrhoea) were not significantly more likely to survive than other Group B puppies. Patients who presented following trauma had a survival rate of 74.1%; this was not significantly different to other paediatric patients. (Table 3). Of the patients who did not survive within Group B, 82.4% were euthanised (Figure 2).
Group C
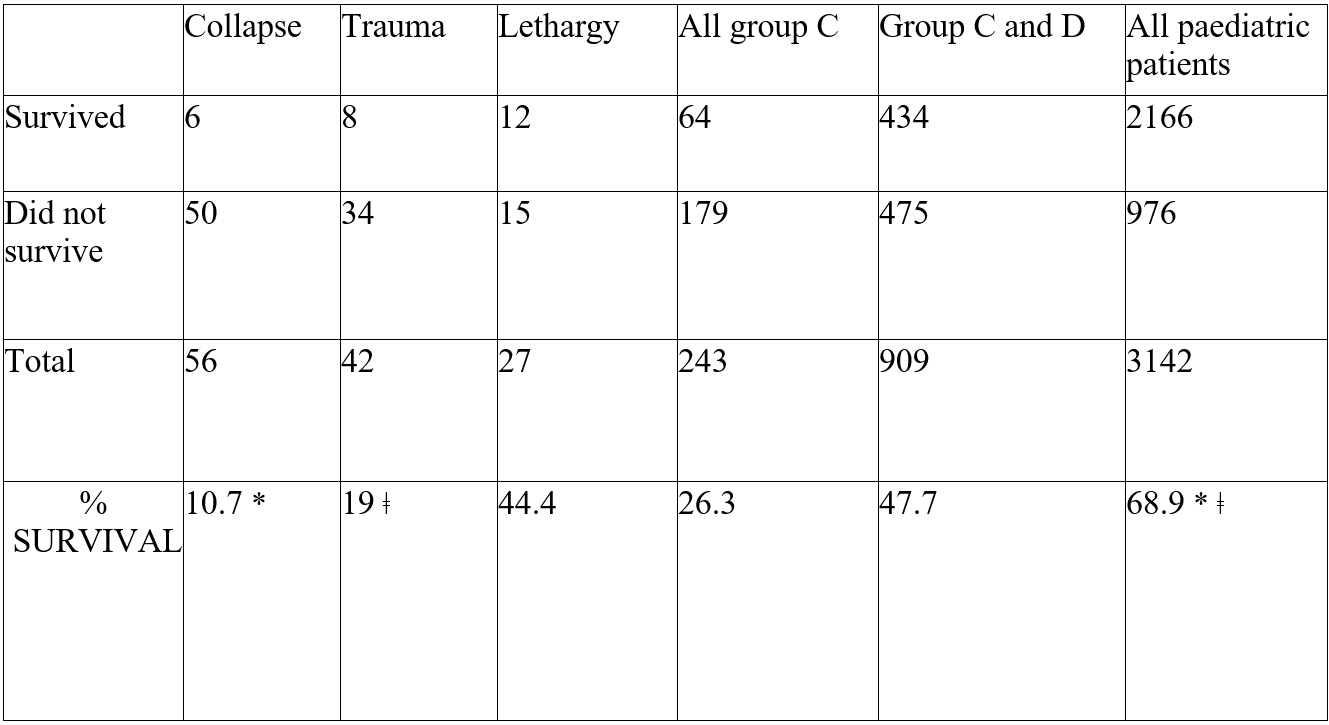
Group C’s overall survival was 26.3%. The most common causes of presentation were collapse (23%), trauma (17%) and lethargy (11%). Feline patients less than 3 months of age had a significantly lower survival rate when compared to other paediatric patients, regardless of species. Within this group, those who presented collapsed and following trauma were significantly less likely to survive than other paediatric patients (group A, B and D), with survival of 10.7% and 19% respectively (p <.001). However, they were not significantly less likely to survive than other patients within the same age group presenting with different complaints. The survival rate (44.4%) of group C kittens presenting with lethargy was not significantly lower than other feline paediatric patients (Table 4). Of the patients who did not survive to discharge within Group C, 90.5% were euthanised (Figure 2).
Group D
Group D’s overall survival was 55.6%. The most common presenting complaints for Group D patients included trauma (15%), collapse (12%) and lethargy (11%). Patients who presented following trauma were significantly less likely to survive than kittens of the same age who presented for other complaints, with a survival rate of 40% (p <.01). Collapsed patients (survival rate of 23%) were less likely to survive than other paediatric patients regardless of species, complaint or age (p <.001). Patients who presented for lethargy had a survival rate of 65.2%; these patients were more likely to survive than other paediatric kittens (Table 5) (p <.005). Of the patients who did not survive to discharge within Group D, 92% were euthanised.
Summary
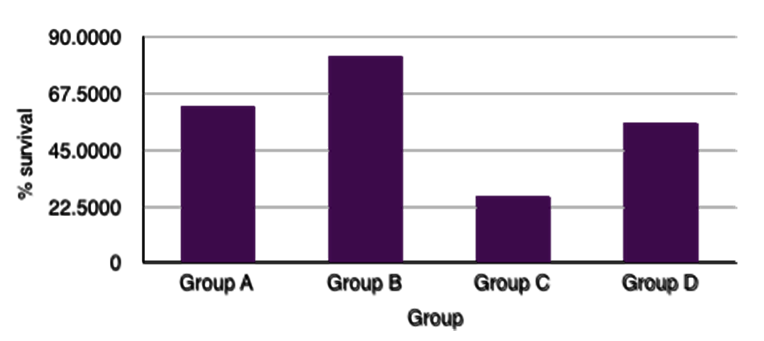
Younger puppies, as a group, had a lower survival to discharge than the older group of puppies (Table 1) (p <.001). Kittens ≤ 3 months of age at presentation (Group C) were less likely to survive to discharge than puppies within the same age range (Group C) (p <.001), with kittens having a relative risk of death of 1.96. Younger paediatric patients (Groups A and C) had a lower survival to discharge than older pediatric patients (Groups B and D) (p <.001), with a relative risk of death of 1.94. Puppies between three and six months of age (Group C) were more likely to survive to discharge than kittens in the equivalent age group (Group D) (p <.001), with a relative risk of death of 2.54. Paediatric kittens (Groups C and D) were less likely to survive than puppies (Groups A and B) (Figure 1) (p <. 001), with a relative risk of death of 2.33.
Our study revealed that older paediatric patients were significantly more likely to survive than younger paediatric patients. As described earlier, paediatric animals have inherently smaller reserve capacities, both in terms of energy stores and in homeostatic function (Gunn-Moore 2006). As these patients age, these capacities increase as their physiology approaches that of their adult counterparts.
The impoverished veterinary literature regarding small animal paediatric medicine may translate into reduced clinician knowledge and familiarity with this population; hence, the low survival rate may therefore also highlight a gap in our understanding of such patients, making their treatment less effective. A future study of a similar population could be designed to determine the impact of clinician experience/qualification upon the survival of these patients.
There are notable species differences, with canine paediatric patients having a much greater chance of survival compared to feline paediatric patients. This finding appears to be universally true, irrespective of the age groups considered. The most common presenting complaints differed between the two species and also differed within species when the two age groups were compared; canine patients were more likely to be presented for vomiting and diarrhoea. However, the third most common complaint differed between the age groups with younger puppies presenting for collapse whilst older puppies presented following trauma.. Feline paediatric patients presented most commonly for lethargy, collapse and trauma; the incidences for each differed between the age groups with trauma being more common within the older feline patients.
One difficulty with the retrospective nature of this study is that patients are placed into distinct categories for their presenting complaint, which is chosen subjectively: for example, patients with gastrointestinal signs could be placed into the collapsed or lethargic categories according to clinician opinion. The ability to record only one presenting complaint is a limitation of the database recording system used in this study and future studies should be designed to overcome this issue. Specific abnormalities such as hypoglycaemia, hypovolaemia, dehydration and hypothermic episodes may accompany many of the recorded presenting complaints and may contribute to hospital presentation as they are a frequent complication in puppies and kittens. However, this study did not allow analysis of the medical records in this level of detail.
Of the most common emergency presentations amongst canine paediatric patients, the collapsed patients had the highest mortality rate as previously described; the survival rate in puppies ≤3 months of age was 22.5%, in feline patients ≤3 months of age was 10.7% and in feline patients 3-6 months of age was 23.2%. This is less than the reported survival of 43% for collapsed adult patients (Firth et al. 2014). A lower survival rate could be explained by the different causes of collapse and the physiologic limitations of paediatric patients. Hypoglycaemia is a commonly reported problem in young small breed puppies and can lead to weakness and collapse (Koenig 2015), with blood glucose levels <2.2mmol/L associated with the development of clinical signs (Bergman 2005). Neonatal and paediatric patients have a higher demand for glucose but are less able to respond to increasing needs for glucose as they have impaired hepatic gluconeogenesis. In addition to this they also have a reduced ability to respond appropriately to hypoglycaemic episodes when calorie intake is reduced for any reason, such as gastrointestinal disease and pain secondary to trauma. Diagnosing hypoglycaemia can be more difficult in this population as their response to a hypoglycaemic episode differs from adults. As this study is retrospective we do not know the percentage of paediatric patients who were hypoglycaemic at the time of presentation. Given the marked effects of hypoglycemia in paediatric patients, assessment of blood glucose level should form part of the minimum database collected for emergency paediatric patients.
Gastrointestinal disease was the most common emergency presentation in canine paediatric patients; survival to discharge increased with increasing age but remained lower than that reported for adult patients (95%) (Firth et al. 2014). Vomiting and diarrhoea are common emergencies in paediatric patients and often occur due to gastrointestinal disease; their limited capacity to cope with illness means that these patients can become rapidly dehydrated and hypovolaemic, which can contribute to collapse. Adult patients will respond to dehydration by reabsorbing water via their kidneys, however younger patients cannot concentrate their urine (Booth 1992; Holster 1971; Fetuin 1991). This can lead rapidly to hypovolaemia secondary to severe dehydration. Adults respond to hypovolaemia by increasing their heart rate and vasoconstriction to maintain blood pressure. In our group of patients, the sympathetic nervous system is immature, and so this response is limited particularly before eight weeks of age; their physiological immaturity may predispose them to increased morbidity and mortality when gastrointestinal disease is present. Determining the level of dehydration is difficult as paediatric patients will continue to have moist mucous membranes whilst being severely dehydrated; they have a higher water content present within their skin than adults, and therefore skin tenting is not a useful part of the clinical examination (McMichael 2015). Difficulties in assessing the level of hydration may contribute to the reduction in survival rate; inadequate fluid resuscitation may exacerbate hypovolaemia in these more vulnerable patients. Infectious disease, parasitic infection, intussusception and foreign bodies are common causes of gastrointestinal disease in puppies and kittens. Paediatric patients are not immunologically or physiologically mature; and as patients mature, survival increases. Another factor associated with this, which may in part also contribute to the differing survival in canine patients ≤3 months and ≤6 months, would be vaccination. Canine parvovirus is a devastating disease with a reported mortality rate up to 91% in untreated patients (Prittie 2004). We would expect that patients between three and six months of age may be vaccinated whilst those <3months of age may be less likely to have completed their vaccination course. There is an expectation that maternally derived antibodies protect younger puppies against disease prior to vaccination. However, it cannot be said that this level of protection is uniform and the timing of susceptibility when these antibodies wane is variable (Day 2014). One study evaluating the risk factors associated with parvoviral enteritis in dogs found that those who were unvaccinated were 1.7 times more likely to require hospital admission than those who had been vaccinated (Hooston 1996). Due to the retrospective nature of this study the vaccination status of our patients is unknown; future prospective studies investigating the underlying cause of diarrhoea and documenting the patient’s vaccination status would be beneficial.
Feline patients were seen more commonly for collapse and trauma. Increasing age was associated with an increase in survival to discharge following trauma. Patients less than six months old had a lower survival rate following trauma than their adult counterparts, reported as 77% (Firth et al. 2014). Feline patients’ small size may make them more susceptible to falling from a height such as from owners arms and they may be more likely to be stepped on in the home.
Another consideration that could account for the low survival is that the small size of these patients makes gaining intravenous access, placement of feeding tubes and general management more challenging. Veins are often small and peripheral blood pressure is lower in healthy paediatric patients compared to the adult dog and cat; in reality intravenous access is perhaps not any more challenging to attain, however, the perception of difficulty may deter repeated attempts to gain vascular access. Determining the success of resuscitation is also more challenging in younger patients as the end-points of resuscitation are not as easily identified. Blood pressure is an important indicator of macro-perfusion, therefore differences between neonatal and adult patients may lead to errors in ascertaining response to resuscitation effort. Micro-perfusion can also be difficult to determine as both puppies and kittens are reported to have higher lactate values than their adult counterparts (McMichael 2005), however a definitive normal reference range has not been established. This may in part explain the low survival rate in paediatric patients presenting collapsed; their response to treatment is inherently more difficult to assess, limiting the practice of goal-directed therapy.
In our study, irrespective of the group, euthanasia was the greatest reason that the patients were ‘non-survivors’; the reasons for this are unfortunately beyond the scope of this study. As previously described financial implications must be considered to be a leading cause, although in the authors’ opinion the decision to euthanise these patients is most likely to be multi-factorial. It is possible that, unfortunately, the human-animal bond may not be as strong with paediatric patients, and so clients may be more inclined to euthanise on financial grounds rather than proceed with veterinary treatment. Euthanasia itself prohibits the development of paediatric veterinary medicine; it limits clinician experience with this age group but also precludes clinical research. As a consequence, anecdotal experience often replaces evidence-based medicine. This is vastly different from our human medicine colleagues who are afforded the opportunity to invest time and finances in treating their patients. The mortality rate following paediatric admission to emergency departments is very low in human medicine - reported as less than 1% in English and Welsh hospitals in 2015/2016 (Keeble 2017).
This study provides important information regarding mortality rates in a large population of paediatric animals presenting as emergencies to multiple out-of-hours clinics. The study is limited by its retrospective nature - no diagnosis was recorded for patients and the single, broad categories for presentation recorded are likely to lead to overlap between groups in terms of the reported complaint. As discussed there is no recording of the reasons for euthanasia such as financial limitations or medical/welfare grounds. Also, as a diagnosis is not recorded we cannot say if the decision to euthanise was based on the patient’s perceived prognosis. As the data was sourced from a large central body obtained from multiple sites it was not possible to ascertain if there were geographical differences in relation to survival. As it was a multi-centre study the clinical outcome may have been affected by differences in clinician approach.
However, despite the limitations, the conclusions of this study are clear: survival of paediatric patients presented to emergency clinics within the UK is low but increases with patient age. Moreover, paediatric feline patients have significantly lower survival rates than canine patients. Further prospective studies are required to fully elucidate the causes of mortality in neonatal and paediatric patients, as well as to investigate whether clinician experience or the application of an algorithmic approach to these patients might alter survival. Such bundles of care have been introduced in both human medicine, the Surviving Sepsis campaign3, and in veterinary medicine, the RECOVER 4 guidelines. The increased evidence base that such research would create, together with its promulgation to practising veterinarians, should drive improvements in clinical care in order to decrease the gap in survival between small animal paediatric patients and their adult counterparts in the future.
The authors declare no conflicts of interest.
Acknowledgement is given to the many and various members of staff at the emergency clinics sampled in this study, for the recording of the clinical data used.
All the supplementary files are available here.
Intellectual Property Rights
Authors of articles submitted to RCVS Knowledge for publication will retain copyright in their work, and will be required to grant to RCVS Knowledge a non-exclusive licence of the rights of copyright in the materials including but not limited to the right to publish, re-publish, transmit, sell, distribute and otherwise use the materials in all languages and all media throughout the world, and to licence or permit others to do so.
Disclaimer
Any opinions expressed in articles and other publication types published in Veterinary Evidence are the author's own and do not necessarily reflect the view of the RCVS Knowledge. Veterinary Evidence is a resource to help inform, and the content herein should not override the responsibility of the practitioner. Practitioners should also consider factors such as individual clinical expertise and judgement along with patient’s circumstances and owners’ values. Authors are responsible for the accuracy of the content. While the Editor and Publisher believe that all content herein are in accord with current recommendations and practice at the time of publication, they accept no legal responsibility for any errors or omissions, and make no warranty, express or implied, with respect to material contained within. For further information please refer to our Terms of Use.